Disior™ is very excited to announce that we are now part of the Paragon 28® family! Together, Disior™ and Paragon 28® will build the Smart 28™. The Disior™ team will be an integral component for SMART 28™, Paragon 28’s ecosystem of enabling technologies for pre-operative planning, intra-operative support, and post-operative evaluation. Disior’s anatomy-specific surgical modules will provide foot and ankle surgeons the objective data needed for the diagnosis and creation of patient-specific surgical plans, and assessment of patient outcomes. Read the full press release concerning the acquisition from Paragon 28® here - ir.paragon28.com/news/news-details/2022/Paragon-28-Announces-Acquisition-of-Disior/default.aspx For today and the years to come, we at Disior™ are committed to providing the same high level of support for research and clinical applications of the Bonelogic™ software that our customers have come to expect. We will keep all our products available for you and your colleagues and will continue to improve our offering. As we develop the Smart 28™ platform, we hope to put it into the hands of our customers to help them analyze, plan and track your patient outcomes. Until then, we are still here for new and existing customers as we were before.
Researchers from the Helsinki University Hospital, the University of Helsinki, and Heidelberg Institute of Global Health (HIGH), Faculty of Medicine and University Hospital, Heidelberg University investigated the factors associated with the choice of treatment in unilateral orbital blowout fractures. This fracture type is usually caused by trauma and affects the bony floor or inner wall of one eye socket. Traditionally, functional impairments such as eye movement disorders and malposition of the globe have guided treatment decisions.
The key results of this study were:
Congratulations to this international team of researchers on their innovative work!Do you want to see how Disior™ CMF Orbital can be benefit your clinical research and practices?
Book a 30 min review of the software. Want to review the software yourself with a 30 day free trial? Request a trial license. Have you got questions about how CMF Orbital works or how to set up research collaborations? Contact our in-house experts at [email protected] The fundamental promise of advanced medical imaging techniques like CBCT and WBCT is improving patient care. With better patient care being achieved through automation of image analysis, increased clinical knowledge and the development of diagnostic metrics. Within extremity orthopedics 3D X-ray techniques are aiding diagnosis and treatment of common foot and ankle conditions like bunions and flat foot. The development and adoption of tools that can automate analysis of 3D medical images is a priority for this community. As automating analysis means removing barriers to both large-scale research projects (that can define normal ranges of bone alignment and objective metrics for defining pathologies and injuries) and use of 3D analytics within clinical practice. Increased collaboration between clinical orthopedic researchers and software developers is vital to achieving the goal of improved patient care.
Dr. Alberto Leardini is author of >190 scientific papers on extremity biomechanics and image analysis, mainly of the foot and ankle. He heads the Movement Analysis Lab group at IOR and is a prominent member of the WBCT society. The first results of the collaboration between Dr Leardini’s group and Disior™, which started at AOFAS 2019, are being presented at i-FAB Congress this April. A similar presentation was also given at the January WBCT virtual meeting, which was covered on our blog and is available to watch on FootInnovate.
Disior™ Bonelogic™ was built specifically to overcome some of issues of automation discussed here. Bonelogic™ takes DICOMs from CT, CBCT or WBCT and generates accurate models and analytics that describe the relationships between bones, in minutes. For example, across the 2600-foot datasets analyzed with Bonelogic™ in 2020 the average time taken for the models and analytics to be generated was 3.1 minutes. If you're interested in learning how Disior's products can aid in your research activities or clinical practice, talk to one of our experts. In a 45 minute meeting we can talk through your current image analysis workflow and discuss what we can do to improve patient outcomes together. 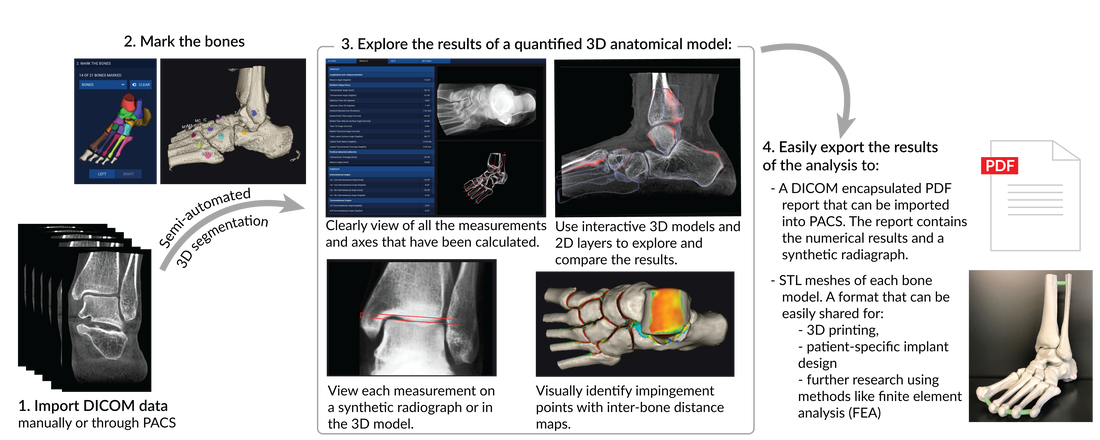  On February 5th, Disior™’s class II medical imaging software device for treatment and surgical planning in the field of orthopedics (foot & ankle and hand & wrist) Bonelogic™ (Bonelogic 2.0) received 510(k) clearance from the US FDA. Within the Planmed-Disior distribution agreement Bonelogic is paired with Planmed’s Verity. The Verity is a low-dose extremity CT scanner which provides 3D images of extremities like the hand & wrist and the foot & ankle. It was the first device in the market able to provide 3D images of the foot & ankle region under natural loading conditions, an imaging technique now commonly termed weight-bearing CT (WBCT). WBCT scanners like the Verity alongside automated medical imaging software like Bonelogic are considered are to be at the forefront of medical innovations for extremity orthopedics. Within the foot & ankle complex, WBCT is a proven tool in both European and American orthopedic clinics for the following common conditions:
Bonelogic™ allows for complete orthopedic characterization of the foot & ankle, as well as the hand & wrist. The software provides mathematical models of a patients’ anatomy and metrics that describe the relationship between bones, which are essential to understanding the degree of pathology or trauma. “The technology within Bonelogic™ means that this type of analysis is completed in minutes. Whereas, in most other medical imaging software it would take hours. Therefore, with Bonelogic™ the barriers to clinical adoption of 3D analytics are removed.” Anna-Maria Henell, CEO, Disior. The magic of combining the distribution of the Verity extremity CT and Bonleogic is that clinical workflows for common hand & wrist and foot & ankle conditions can be optimized. Reducing the workload of radiologists and clinicians.
Disior Oy and Planmed
Disior Oy's mission is to provide medical professionals with the diagnostic information they need to deliver perfectly-tailored treatments to every patient. To do this Disior develops novel ways to automate the analysis of bones and soft tissue, linking medical doctors with engineers and mathematicians. The company owners include both leading orthopedic and maxillofacial surgeons as well as technology visionaries. Planmed Oy dedicates its effort to the development, manufacturing and marketing of advanced imaging equipment and accessories that provide a unique combination of image quality and ease of use for medical imaging professionals. The company offers products for mammography and orthopedic imaging that are well-known for imaging performance, user-friendliness and good ergonomics. Since 1989, Planmed systems have provided tools for healthcare professionals in over 70 countries worldwide. Planmed Oy is part of the Finnish Planmeca Group, which operates in the field of health care technology. Disior Bonelogic® has the potential to revolutionize the diagnosis and treatment of patients suffering common extremity injuries and diseases.
“Disior and the Disior Bonelogic software allow us to perform quick and automatic bone segmentation, as well as provided us with a thorough assessment of the relationship and three-dimensional orientation of the tarsal bones. It is a game-changer and will become the standard in the assessment and treatment of patients.” |










 Iowa Team, photo courtesy of Dr Dibbern | 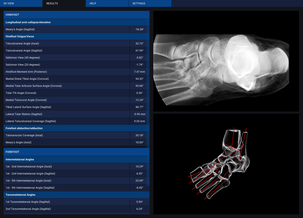 Example of automated 3D analysis results possible in Bonelogic |  Iowa Team in action, photo courtesy of Dr Dibbern |
Collaborative research is at the heart of the development process at Disior. Partnerships with Finnish and European Hospitals and Universities have proved extremely beneficial to the development of our products. For example, testing and defining clinically relevant measurements that describe the hand and wrist, the other extremity currently covered by the Bonelogic software.
| To Disior CEO Anna-Maria Henell, the strategic partnership with the University of Iowa’s OFIRL means that “we can work closely with a world-class team of experts to fine-tune our 3D medical imaging software, Bonelogic, for clinical practice in the USA. This collaboration will also allow us to quantify the benefits of the software for research and clinical practice. We aim to reduce the work-load of clinicians and to advance understanding of complex 3D anatomies so that patients get the right treatment every time, this partnership will help us achieve this goal.” |  Disior CEO Anna-Maria Henell |
If you're interested in discussing research projects, collaborations or are just intrigued to see what role Disior's innovative medical imaging software can play in your clinic or research group contact us.
On Saturday 16th January the Weight-Bearing Computed Tomography Society held their 2nd Annual International Meeting. The recordings of each talk are being made available via the FootInnovate platform. If you don't know which talks to watch or aren't a member of FootInnovate then this guide synthesises the key themes of the talks and highlights key speakers for each topic.

| “The WBCT Society is currently the only scientific society in the world with more publications than members.” – Associate Professor Martinus Richter, MD. |  |
The International WBCT Society is an academic society focused on enhancing diagnosis and understanding of weight-bearing foot and ankle conditions. The IWBCT promotes dialogue and collaboration on weight-bearing CT research initiatives, through events like the 2nd International WBCT Society Virtual Meeting. The goal of the society is to help create standardised clinical protocols for weight-bearing CT measurements and analysis.
Theme 1. Innovation
 Francois Lintz (President-Elect, WBCT Society) opened proceedings with Figure 1, which shows that the amount of WBCT research has quadrupled since Weight-Bearing Computed Tomography (WBCT) scanners came onto the market. This rise in publications is not just an indicator of the importance of the technique to answer scientific questions but also “means better understanding of the complex 3D anatomies – and ultimately better outcomes for patients”. | 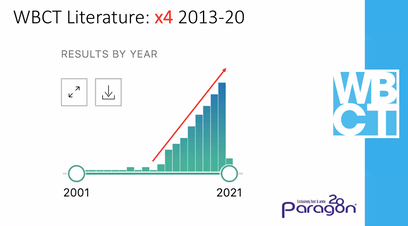 Figure 1. WBCT literature through time, from Dr Lintz's presentation. |
This link between research and clinical practice pervaded all talks at the meeting. In particular, the talks by Dr’s Ellis and Welcks made it clear that WBCT is becoming the standard for assessing the following foot and ankle conditions in both Europe and the USA:
The main advantages of WBCT for these conditions being that clinicians can:
- Hallux Valgus/HR
- Syndesmotic Injuries and Instabilities
- Progressive Collapse Foot Deformity (previously known as Acquired Adult Flatfoot Deformity)
- Ankle, hindfoot and midfoot arthritis
The main advantages of WBCT for these conditions being that clinicians can:
- Easily assess the degree of deformity and bone positioning under natural loading conditions, even in complex cases where the pathology is multiplanar. Talks by Drs Haapasalo, Day, Wellenberg and Conconi assessed anatomical differences between CBCT and WBCT imaging.
- Improve surgical planning with accurate 3D anatomical data and models.
- Use post-operative scans to assess treatment efficacy and healing.
- Prevent unnecessary surgical intervention in borderline cases where a diagnosis is uncertain.
- Save costs and time by removing the need to perform standard CT, CBCT or plain X-rays.
- Make comparisons to an unaffected side using bilateral WBCT systems.
- Conduct large scale studies that improve medical knowledge and patient treatment.
One other clear outcome from the meeting was the rising use of WBCT for patients with hip and knee problems like patella instability (Dr Belvedere), knee arthritis (Dr Segal) and hip preservation (Dr Willey). Across these presentations, WBCT: enhanced understanding of kinematics, increased detection of arthritis and allowed for joint space quantification. Further work in these two anatomies is sure to bring about better patient care and quality of life improvements.
Talks concerning these topics:
Talks concerning these topics:
- Dr Scott Ellis - Hospital for Special Surgery, NYC, USA
- Dr Matthew Welcks – Stanmore Hospital, London, UK
- Dr Claudio Belvedere - Instituto Ortopedico Rizzoli di Bologna, Itay
- Dr Neil Segal - University of Kansas, USA
- Dr Michael Willey - University of Iowa, USA
“So pleased at the multidisciplinary nature of this meeting and we are excited to see radiologists and knee and hip specialist join the WBCT community”- WBCT Society President Alexej Barg MD |  |
Theme 2. Advances in 3D Analytics
A second key theme of the meeting was the analysis of three-dimensional medical images. Acquiring 3D data is just the first step in the process for both clinical and research workflows. Analyzing this data is the next step. That starts with the segmentation of bones and then the measuring distances and angles relevant to the diagnosis at hand.
 | “Large scale studies of 3D measurements are not viable given long processing times for segmentation”- Dr Ruud Wellenberg, MD |
Dr Wellenberg’s excellent study comparing 2D vs 3D, and CBCT vs WBCT data highlighted a common drawback to analysing 3D data- the time involved in segmentation. He reported spending 6 hours per patient manually segmenting data, slice by slice. Dr Wellenberg was not alone, talks by Drs Conti and Leardini (among others) also mentioned the prohibitive time expense that segmentation requires. In contrast, the time savings discussed by Drs Burssens, Haapasalo, and Leardini, who used Disior’s automated medical imaging software stood out (e.g. Figure 2).
"Disior's a real time-saver, 20 minutes per case with automated measurements as opposed to 6hrs just for segmentation”- Dr Arne Brussens, MD
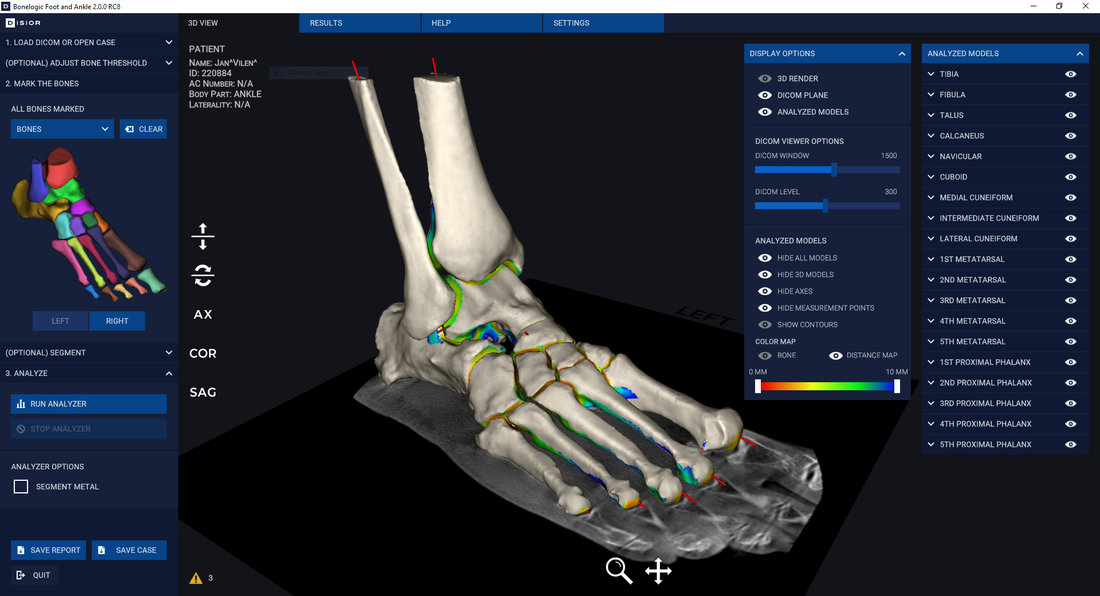
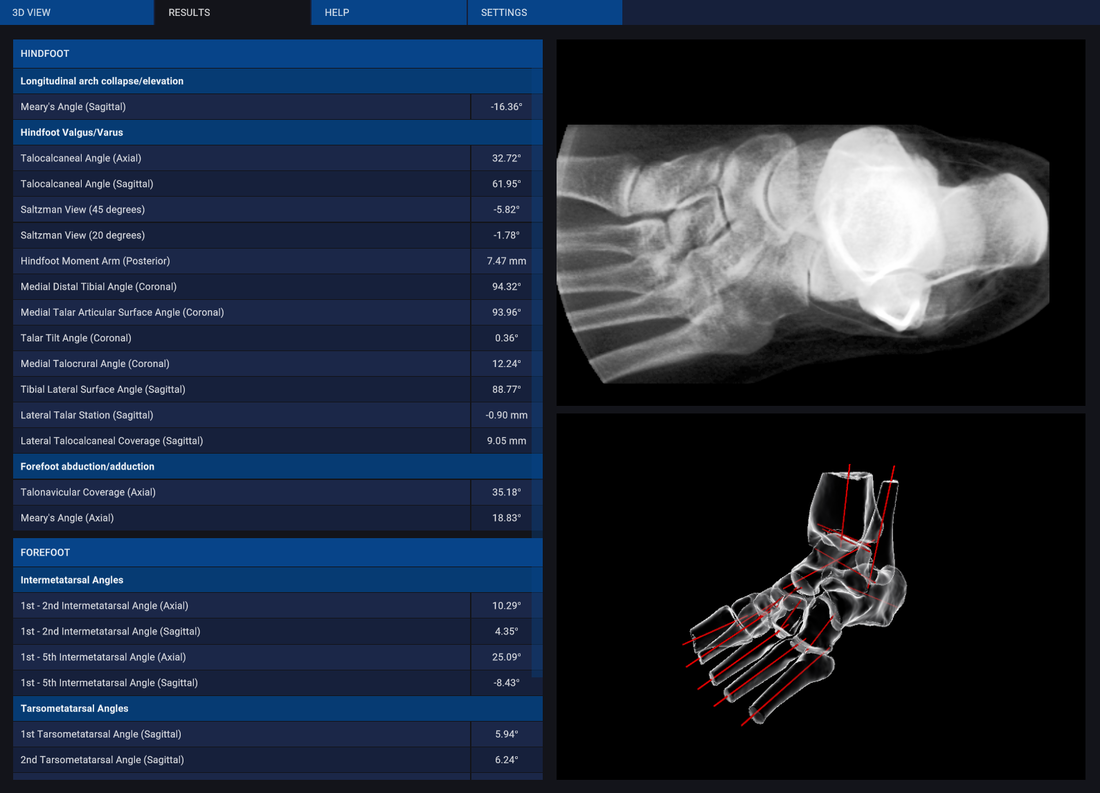 Figure 2. Example of the type of analysis that can obtained using Disior Bonelogic Ortho Foot and Ankle in minutes as mentioned by Drs Brussens, de Cesar Netto and Leardini. |  Figure 3. Example of joint space mapping as mentioned by Drs Haapasalo and Vivcharenko. Currently available in Disior Bonelogic 2.0. |
Drs Haapasalo and Vivtcharenko were the first female speakers at any IWBCT meeting. Both of their talks focused on ways to define joint spacing in 3D (e.g. Figure 3). Joint spacing is a key metric for assessing many foot and ankle conditions, like syndesmotic instabilities and flat foot. By investigating this parameter across healthy individuals and those presenting with different types and degrees of pathology, Drs Haapasalo and Vivtcharenko showed how this type of research can directly impact on clinical practice. Dr de Cesar Netto's talk was also concerned with using 3D analytics to classify the degree of pathology, so that patient groups are more easily defined. The ultimate goal for most research presented at the meeting is a move in clinical practice towards early identification and mitigation of dis-ease.
Some very interesting questions arose in the breaks and we at Disior will be releasing articles about the following:
- What is the effect of smoothing on the accuracy of 3D models?
- How reliable is automated segmentation of medical imaging data in complex cases?
| Talks concerning these topics:
| |
Theme 3. Validation & Standardization
| The final theme that emerged from the talks and discussions between sessions concerned validation and standardization of measurements made in 3D. Two talks approached this topic in a very systematic way for the same problem- metatarsal pronation: 1) Dr Conti evaluated four different methods for measuring pronation, including a 2D vs 3D comparison, and 2) Dr Miller et al., tested how the viewing angle affects the measurement of pronation. These two presentations effectively exemplified that how and where you measure affects the outcome. That when it comes to clinical significance there is an obvious limitation - how do these types of measurements vary in healthy people? | 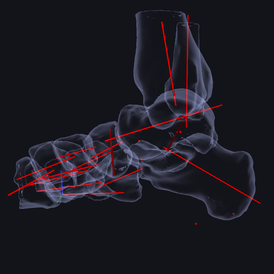 Figure 4. Image of an analyzed foot and ankle model. Where we define the measurement points and landmarks matters. For us at Disior, we use points that can be mathematical defined and found reliably. |
 | "At this time, there is no 'ideal' post-operative pronation ”- Dr Matthew Conti, MD |
Dr Leardini’s talk demonstrated a current large-scale study being undertaken to address these issues and is well worth listening to. The paper from this study will go into details of time savings and measurement reliability. Dr Leardini also welcomes everyone working in the foot and ankle field to participate in the measurements survey being hosted by the WBCT.
The survey aims to garner a wide range of responses to help guide the development of measurement standards and definitions for foot and ankle conditions. By taking part in the survey you will be actively helping to advance clinical 3D analytics of the foot and ankle and ultimately patient care. The results of the survey will be published by the WBCT Society.
The survey aims to garner a wide range of responses to help guide the development of measurement standards and definitions for foot and ankle conditions. By taking part in the survey you will be actively helping to advance clinical 3D analytics of the foot and ankle and ultimately patient care. The results of the survey will be published by the WBCT Society.
Overall, the strategies to address validation and standards that seemed to resonate with the attendees were ones involving a high degree of repeatability, automation and objectivity (like Disior) or integration into existing systems (like PACS).
Talks concerning these topics:
We at Disior were proud to sponsor the 2nd International WBCT Society Virtual Meeting alongside Planmed, Footinnovate, Curvebeam and Carestream.
Talks concerning these topics:
- Dr Michele Conconi - University of Bologna, Italy
- Dr Alberto Leardini - Instituto Ortopedico Rizzoli di Bologna, Itay
- Dr Jonathan Day - University of Iowa, USA
- Dr Matthew Conti - Hospital for Special Surgery, NYC, USA
- Dr Mark Miller - Allegheny General Hospital, USA
We at Disior were proud to sponsor the 2nd International WBCT Society Virtual Meeting alongside Planmed, Footinnovate, Curvebeam and Carestream.
About Us
Disior makes 3D medical imaging software that segments and analyzes 3D anatomies like the foot and ankle. Our software products are CE marked and regulated as medical software devices meaning that the 3D models and analytics have a high degree of reliability and accuracy. If you want to see what we can offer you in terms of automating 3D medical image analysis, get in contact to arrange a demo and a free trial.
 RSS Feed
RSS Feed